
Benchmarks and Best Practices for Acute and Extended Health Care Facilities:
A Guide for Energy Managers and Finance Officers
Please note:
This publication may refer to programs that are no longer available. For current information, please visit ecoENERGY or contact us.
Table of Contents
3.0 Energy Use in Health Care Facilities
5.0 Energy Savings Mean Dollar Savings
1.0 Introduction
1.1 Aim of This Guide
This Guide is intended to help energy managers, finance officers and others who have responsibility for energy use in acute and extended health care facilities compare the energy performance of their facilities with that of others. It may also be of use to directors and other individuals who are more broadly involved in managing health care facilities.
Best practices to improve the energy efficiency of health care facilities are outlined.
The objective of this Guide is to foster a commitment to energy efficiency by providing health care organizations with information on energy efficiency and energy management.
The broader goal of this Guide is to assist the Energy Innovators Initiative, a program of Natural Resources Canada's Office of Energy Efficiency, in its mandate to promote energy efficiency and reduce greenhouse gas emissions that contribute to climate change.
This Guide covers two types of health care facilities:
- acute care
- extended care
2.0 Energy Management
2.1 Why Is Energy Management Important?
Energy management ensures that energy use and costs are as low as possible while maintaining high standards of comfort, service and productivity. The various benefits associated with improving energy management include the following:
- improved comfort
- reduced operating and maintenance costs
- reduced system and equipment failures
- improved building value
- improved productivity of equipment and staff
- increased building and equipment life
- reduced energy consumption
- improved environmental performance
2.2 Why Analyse Energy Use?
Analysing energy use and energy use patterns allows you to identify areas of inefficiency in your operations. You can then develop and implement an energy management plan to improve your facility's performance and reduce costs.
A good starting point for creating an energy management plan is to develop a baseline of your facility's energy consumption. This usually involves identifying where and at what rate energy is used, areas of energy waste and potential energy-saving measures.
When conducting an energy use analysis, it is useful to understand industry trends, patterns and superior performance values. The benchmarks and best practices outlined in this Guide are based on a 1998 survey, conducted jointly by the Energy Innovators Initiative and the Canadian College of Health Service Executives, about energy consumption in health care facilities across Canada.
2.3 Economic Impacts of Energy Efficiency
A facility's energy performance has a significant impact on its bottom line. If money is wasted due to energy inefficiency, its overall financial performance suffers.
In addition, a building's energy performance is closely linked with its indoor environment and air quality, which affect occupant comfort and productivity.
2.4 Factors That Affect Energy Use in Health Care Facilities
The following are the primary factors that affect energy consumption in a health care facility:
- source of energy used (natural gas, coal, hydro generation)
- facility size
- age of facility
- hours of operation
- climate
- heating, ventilating and air-conditioning (HVAC) systems
- budget for energy management
The following factors are considered to be secondary when analysing a health care facility's energy consumption:
- type of on-site facilities, including
- kitchens
- laundry areas
- incinerators
- burn units
- laboratories
- emergency services
- hospital equipment
- building envelope (including window conditions)
- lighting type and illumination level
3.0 Energy Use in Health Care Facilities
3.1 Characteristics of Existing Health Care Facilities (Survey Results)
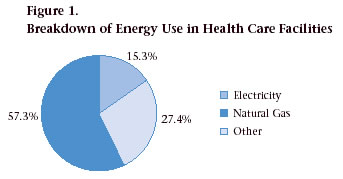
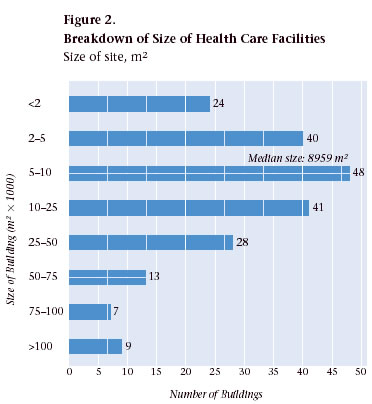
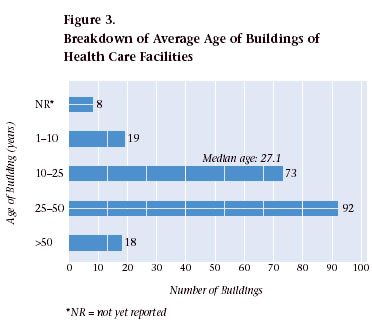
In this Guide, data are based in part on a survey conducted in 1998 of health care facilities across Canada. Of the 879 facilities surveyed, quantitative data were collected from 222 facilities. Additional data were also gathered through discussions with representatives from a range of regions and from health care managers of individual facilities.
The following graphs are based on the results of the survey and illustrate basic characteristics about health care facilities in Canada.
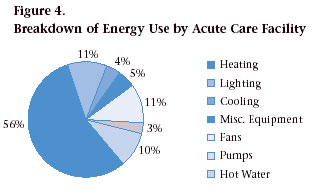
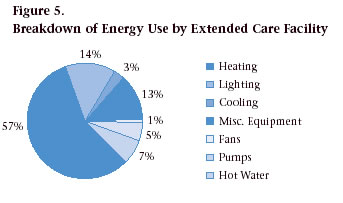
3.2 Energy Use Patterns in Acute and Extended Care Facilities (Modelling)
Using modelling software, energy consumption by building in acute and extended care facilities was determined.
Figures 4 and 5 illustrate a breakdown of total energy use and individual end-use intensities for these facilities.
4.0 Benchmarks
4.1 What Are Benchmarks?
Benchmarks allow organizations to monitor their energy management practices and performance and to compare them with those of other buildings and organizations and against specified performance standards.
Energy management benchmarks compare a building's annual energy consumption with that of similar buildings. Benchmarks can help to
- provide a snapshot of individual performance compared with "the average" and "the best"
- establish trends, evaluate historical performance and plan future activities and operations
- establish performance triggers and targets to minimize risk more easily and effectively
- generate organizational motivation to improve a facility's energy performance
- demonstrate the link between specific factors (energy drivers) and energy performance
- determine more easily whether operational changes are necessary, without having to conduct a full audit
- disseminate information in a simple manner that is understandable by both technicians and managers
4.2 Calculating a Benchmark for Your Facility
A useful benchmark quantifies energy consumption in terms of energy intensity (i.e., units of energy consumed per floor area per year). Although whole-building measures such as these have limitations, they can be useful in providing an initial assessment as to how a building compares with others.
Calculate a benchmark for your facility using Table 1 and the instructions that follow.
| Source | Conversion | Equivalent kWh (ekWh) |
|---|---|---|
| Electricity | kWh x 1 | = ________ ekWh |
| Natural Gas | m3 x 10.33 | = ________ ekWh |
| GJ x 277.78 | = ________ ekWh | |
| Steam | kg x 0.154 | = ________ ekWh |
| Propane | litres x 7.09 | = ________ ekWh |
| #2 Oil | litres x 10.74 | = ________ ekWh |
| #6 Oil | litres x 11.25 | = ________ ekWh |
| Diesel | litres x 10.74 | = ________ ekWh |
| Wood | tonnes x 3876.70 | = ________ ekWh |
| Gasoline | litres x 9.63 | = ________ ekWh |
| 1. Calculate the total floor area of your facility in square metres: ___________ m2 | |||
| 2. Determine your facility's annual energy consumption and costs, and convert annual energy consumption into ekWh: | |||
| Electricity | ________ kWh | ________ kWh | $________ |
| Natural gas | ________ m3 x 10.33 = | ________ ekWh | $________ |
| #2 Oil | ________ L x 10.74 = | ________ ekWh | $________ |
| #6 Oil | ________ L x 11.25 = | ________ ekWh | $________ |
| Other* | ________ | ________ ekWh | $________ |
| Total: ________ ekWh | $________ | ||
| 3. Calculate your facility's energy intensity and its cost of consumption: Total ekWh/m2: ________________ $/m2: ________________ | |||
| 4. Compare your facility's energy intensity with those of other health care facilities listed in Figures 6 through 11. | |||
| * This includes steam, propane, diesel, wood and gasoline. | |||
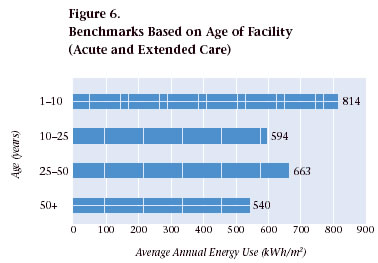
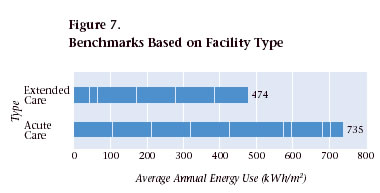
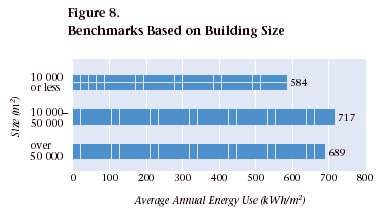
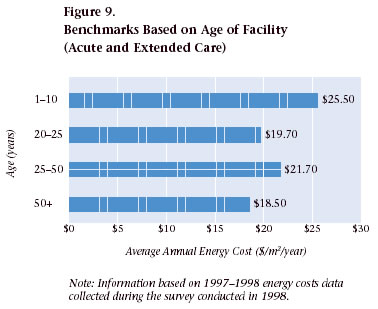
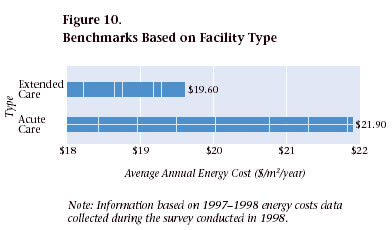
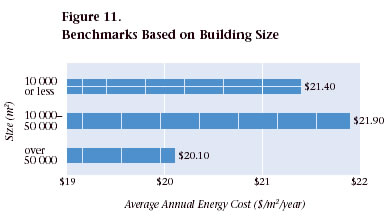
4.3 Benchmark Scales
The following benchmark scales are based on survey information on energy use in the health care sector and from the modelled facilities.
Benchmarks for Existing Facilities (Acute and Extended Care)
Energy Use
Energy Costs
5.0 Energy Savings Mean Dollar Savings
After you have compared your facility's energy consumption with the benchmark data, you should have a good idea as to how your health care facility compares with others. This analysis will help reveal where inefficiencies exist and identify possible opportunities to improve your organization's energy efficiency.
Based on these results, you may want to develop a strategy to increase the level of energy efficiency in your organization. Your plan should incorporate a variety of measures, including capital investments and low and no-cost initiatives.
Low and no-cost initiatives are an important component of an energy-saving strategy. They can generate significant savings and can provide the impetus for senior management to approve more capital-intensive measures.
To help you set your plan in motion – and to help obtain approval to implement energy-saving retrofits – information on your organization's potential rate of return for purchasing new, energy-efficient equipment has been provided in Table 2.
The first column indicates the simple payback period of the investment and is defined as follows:
the value of the project
__________________
the cost of the project
The life cycle is the time (in years) the equipment will be included as part of your energy conservation project.
For example, if your organization invested in an energy-efficient lighting system that cost $15,000 with annual energy savings of $3,000, your simple payback would be five years. If your lighting system had a 10-year life cycle, your internal rate of return would be 15 percent, or the equivalent of earning 15 percent on your investment.
| Simple Payback Period (years) |
Life Cycle (years) | ||||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 10 | 15 | |
| Rate of Return (percent) | |||||||
| 1 | 0 | 62 | 84 | 93 | 97 | 100 | 100 |
| 2 | 0 | 23 | 35 | 41 | 49 | 50 | |
| 3 | 0 | 13 | 20 | 31 | 33 | ||
| 4 | 0 | 8 | 21 | 24 | |||
| 5 | 0 | 15 | 18 | ||||
| 6 | 10 | 15 | |||||
| 7 | 7 | 12 | |||||
| 8 | 4 | 9 | |||||
| 9 | 2 | 7 | |||||
| 10 | 0 | 6 | |||||
6.0 Best Practices
6.1 What Are Best Practices?
In any benchmark comparison, facilities with an energy consumption rate at or near the minimum could be considered to be applying current best practices.
The term "best practices" refers to proven industry solutions for improving performance. Best practice standards to improve the energy efficiency performance of new buildings in Canada are established by National Research Council Canada's Model National Energy Code for Buildings (MNECB). This code sets minimum energy efficiency standards for commercial building construction in Canada.
The Commercial Building Incentive Program, administered by Natural Resources Canada's Office of Energy Efficiency, offers a financial incentive for the incorporation of energy efficiency features into new building designs. To qualify for the incentive, a building must be 25 percent more efficient than one built to the MNECB.
In this Guide, best practices are considered to represent measures that, when successfully implemented, lead to reductions in energy consumption in economical and achievable ways.
6.2 Best Practices for Improving Energy Performance in Acute and Extended Care Facilities
Improve Building Envelope Characteristics
Building envelope improvements are most cost-effective when they are conducted as part of new construction or retrofit initiatives.
- Upgrade insulation levels as part of other projects (e.g., new construction, re-roofing).
- Check insulation for condensation and water penetration.
- Insulate roof voids.
- Draft-proof windows and doors.
- Install double- or triple-glazed windows, preferably with low emissivity (low-E) glass.
- Install automatic doors in areas where external doors are frequently left open.
- Install plastic secondary door curtains inside delivery doors.
Improve Lighting Design and Efficiency
- Install energy-efficient lighting fixtures.
- Install lighting controls and occupancy sensors in staff areas.
- Replace incandescent lighting with compact fluorescent bulbs.
- Rely on daylight for interior illumination.
- Convert exit signs to light-emitting diode (LED) fixtures.
- Use metal halide or sodium discharge lamps for outside areas.
Improve Efficiency of HVAC Systems
Because space heating represents one of the largest end-uses in acute care facilities, it also offers the largest potential for energy savings.
- Install high-efficiency condensing boilers.
- Recover excess heat from ventilation systems through high-efficiency axial fans. This is a very successful energy-saving measure in health care facilities because of their continuous operation.
- Consider alternative sources of energy, such as ground-source heat pumps.
- Install high-efficiency chillers.
- Rebalance, reduce and schedule flows of supply, return and outside air. Eliminate oversizing by removing HVAC use where possible.
- Eliminate oversizing of pump capacity on water heating, glycol and chilled water systems. Remove secondary booster pumps, if possible.
- Convert mixing boxes from constant to variable volume.
- Add direct digital controls to thermostats and lighting.
- Install variable frequency drives on principal motors.
- Convert from air-wash systems to steam humidification.
- Combine steam systems where possible.
- Eliminate once-through cooling systems (i.e., add cooling towers).
- Use steam condensate for hot water preheating.
- Maximize free cooling.
- Carry out waste incineration heat recovery by installing waste heat recovery units that are separate from the incinerator.
Water and Sewer Management
Substantial savings opportunities are available through conservation activities.
- Contract out laundry services.
- Schedule lawn watering.
7.0 Case Studies
This section presents case studies of energy efficiency measures implemented by various health care facilities across Canada.
7.1 Case Study No. 1: Walter C. Mackenzie Health Sciences Centre, Edmonton, Alberta
Overview
- The facility, completed in 1986 at a cost of $900 million, currently has over $100 million worth of new projects under way, including a new emergency wing.
- It has an annual energy budget of $5.7 million.
- Its energy efficiency target is to reduce 2002 consumption levels to 15 percent below 1999 levels.
- Increased use and medical advances, especially diagnostic imaging, are driving most of the changes in the facility.
- A unique building feature is the mechanical/electrical service spaces between floors. Open-web steel joists, 2.5 m (8 ft.) high, were used to construct the floors, and the ease of access makes it easy to retrofit the building.
Energy Systems and Retrofits
Overall Facilities Management
- Master specifications must incorporate energy efficiency.
- Pilot projects are used to prove a technology before it is implemented on a broad scale.
- Awards are used to communicate and motivate management and staff.
- High utility bills help focus the organization's attention.
- Well-trained and motivated staff is critical to the success of an energy efficiency program.
Lighting
- Metric pans have been retrofitted with 0.6-m by 0.9-m (2.0-ft. by 3.0-ft.) T-8 tubes with reflectors.
- Out of more than 40 000 light fixtures, 9000 have been retrofitted.
Building Envelope
- Stairwells have been reinsulated and resealed.
- Windows in the main building and in the atrium need to be resealed.
- The atrium has a very large barrel-vault skylight of slightly tinted glass. Any retrofit would likely be prohibitively expensive.
System Balancing
- Since 1994, the water side and air side of the entire building have been re-balanced as an ongoing project, which has reduced total flows considerably.
- The facility started out with continuous 800-Pa duct static; its standard now is about 500 Pa during the day and 200 Pa at night.
Direct Digital Control of Mixing Boxes
- Because the building was built in two phases, one part has a dual duct system and the other part has a variable air volume system with reheat.
- There are 2000 mixing boxes, and although 1550 are still pneumatically controlled, 450 have been converted to direct digital control.
Variable Frequency Drives on Return Fans
- The installation of variable speed drives to fan and pump motors has proven to be an extremely successful program.
- Existing supply fans have variable pitch fan blades that can achieve high efficiencies over a fairly wide range. Return fans equipped with variable inlet vanes have been converted to variable frequency drives.
- Variable speed drives have been installed to regulate flow control and can be applied to standard off-the-shelf AC motors.
Pump Capacity on Chilled Water System
- After testing and re-balancing all riser and coil flows, it was determined that all secondary booster pumps could be removed.
- This consisted of removing 28 booster pumps, one for each air-handling unit, ranging in size from 7 to 15 hp.
Variable Frequency Drives on Primary Heating, Chilled Water and Glycol Pumps
- After testing and re-balancing all riser and coil flows, it was determined that all primary pumps were oversized. For example, the glycol system originally ran two 7.5-hp pumps continuously. Now the system operates with only one 7.5-hp motor on a variable frequency drive.
Conversion From Air-Wash to Steam Humidification
- In each of the 28 main air-handling units, spray-type air washers were replaced with steam humidification.
- This improved indoor air quality, provided better control of humidity levels and fewer swings and eliminated maintenance and electrical costs for the water circulation pumps, which resulted in savings of $100,000 in water treatment chemicals and $51,000 in demineralization costs.
Elevators
- Nineteen elevators are being converted to variable frequency drives. Although energy savings from this project are low, there are savings in floor space and initial costs of equipment.
Shutdown of Atrium Air-Handling Units
- Originally, the atrium was heated by 10 air-handling units equipped with 5-hp to 7-hp supply fan motors and 2-hp to 3-hp return fan motors. These units operated continuously.
- Now the atrium is heated through heat losses from the main building. The air-handling units are used only to maintain a positive 10-12 Pa pressurization on the lower floor during the winter.
Heat Recovery
- Air-to-air heat recovery wheels were retrofitted into the air-handling units. This has been a hugely successful pilot project.
Peak Shaving and Supply Side Management
- The Centre purchases power, steam and chilled water from the University of Alberta power plant. There is a reciprocal agreement with the power plant to provide peak shaving for the University by using the Centre's diesel backup generators.
- The Centre pays negotiated prices based on the volume of steam and chilled water supplied, not the Btu content.
Water and Sewer Management
- Water and sewer billing to the Centre has dropped considerably in recent years because of conservation activities and by contracting out laundry and incineration functions.
- Although the incinerator presented a large opportunity for heat recovery, funding for the upgrade was not available.
For more information, contact
Doug DunnManager, Building Operations
Walter C. Mackenzie Health Sciences Centre
University of Alberta Hospital
Capital Health Authority
8440 – 112 Street
Edmonton AB T6G 2B7
Tel.: (780) 407-8179
Fax: (780) 407-8895
E-mail: ddunn@cha.ab.ca
Web site: www.cha.ab.ca
7.2 Case Study No. 2: Regina Health District, Regina, Saskatchewan
Overview
Regina Health District consists of two large hospitals:
Pasqua Hospital
- It has 267 beds.
- The Alan Blair Cancer Centre consists of two buildings: one with 52 500 m2 (565 000 sq. ft.) and the other with 75 000 m2 (80 000 sq. ft.).
- Services include general, orthopaedic, urology, intensive care and cardiology.
- Over the last five years, it has renovated 43 000 m2 (464 000 sq. ft.), or 40 percent of total facilities, and has demolished 11 500 m2 (124 000 sq. ft.).
Regina General Hospital
- It has 635 beds.
- It has 88 600 m2 (954 000 sq. ft.) over six floors, including additional wings throughout the hospital.
- Services include maternity, neonatal intensive care, dialysis, neurology surgery and a trauma centre.
- Over the last five years, it has renovated 52 400 m2 (564 000 sq. ft.), or 65 percent of total facilities, and has demolished 21 400 m2 (230 000 sq. ft.).
Energy Management and Retrofit Measures
- Renovations featured $1.7-million worth of energy-efficient features.
- Energy features were based on life-cycle costs and a projected 4.1-year simple payback.
- Features include the following:
- Installed stack economizers to collect heat from boiler combustion exhaust.
- Replaced electrical centrifugal chillers with gas-based absorption chillers.
- Installed variable speed drives on fans and pumps.
- Replaced a boiler at Regina General Hospital with a high-efficiency unit.
- Installed T-8 lighting and electronic ballasts in new construction and renovated areas. Currently replacing T-12 lighting and magnetic ballasts in old portions of the hospitals.
- Installed a building automation system with direct digital controls in Pasqua Hospital and Regina General Hospital.
- Consolidated all controls in order to be operable by one system.
- Installed dual duct system and radiant heating on glycol loop.
- Installed variable air volume distribution boxes in every room.
- Upgraded insulation to code in new/retrofit construction and installed doublepane, low-E argon windows.
Energy Savings
Pasqua Hospital
- Pre-retrofit energy intensity: 110.75 kWh/sq. ft. (1995-1996).
- Post-retrofit energy intensity: 97.94 kWh/sq. ft. (1999-2000).
- Overall drop in energy consumption: 11.6 percent (much higher reduction for newly renovated portions only).
Regina General Hospital
- Pre-retrofit energy intensity: 96.04 kWh/sq. ft. (1995-1996).
- Post-retrofit energy intensity: 85.14 kWh/sq. ft. (1999-2000).
- Overall drop in energy consumption: 11.4 percent (much higher reduction for newly renovated portions only).
Future opportunities
- Installing better controls (i.e., scheduling) to get greater energy savings.
- Establishing a computerized maintenance program to improve maintenance and the operation of the combined heating plant.
- Reducing current air volumes.
- Investigating the use of lighting controls.
- Instituting an energy-efficient equipment procurement program.
- Implementing an energy efficiency education program for housekeeping staff.
For more information, contact
Peter WhitemanEnergy Centre Manager
Regina Health District
2180 – 23rd Avenue
Regina SK S4S 0A5
Tel.: (306) 766-5365
Fax: (306) 766-5414 E-mail: pwhiteman@reginahealth.sk.ca
Web site: www.reginahealth.sk.ca
7.3 Case Study No. 3: St. Paul's Hospital, Vancouver, British Columbia
Overview
1894 – the original wooden structure was built (it has since been demolished)
1912 – the Burrard Building Centre Block and power house were constructed
1930 – the Comox Building and Burrard Building North Wing were constructed
1939 – the Burrard Building South Wing was constructed
1946 – a major addition to the Comox Building was constructed
1949 – the Burrard Building East Wing was constructed
1953 – the Burrard Building West Wing was constructed
1961 – the McDonald Building was constructed and the power house was upgraded
1979 – the Providence Building Phase I was constructed
1986 – the emergency ward was constructed (as an addition to the Burrard Building Centre Block)
1989 – the Providence Building Phase II was constructed
1999 – St. Paul's Hospital had the third lowest physical plant costs in Canada
Energy Retrofit Measures
Energy Supply
- In 1982, the hospital joined the district steam heating system, and the power house was decommissioned.
- Electric power is supplied by BC Hydro.
- The budget for the department in 2000 was $4.3 million.
- The budget for energy in 2000 was $1.8 million.
Energy Performance Contract
- The project cost $3 million, based on a 10-year payback period.
- The project started in November 1998 and was completed in May 2000 (18 months).
- The primary focus was on the Providence buildings.
- Projects included the following:
- Upgrading existing controls.
- Installing variable frequency drives on supply, return and exhaust fans and glycol pumps.
- Redesigning and replacing existing lighting system with electronic ballasts, T-8 lamps and reflector kits.
- Re-balancing air flows to match the reduced cooling load and the new lighting system and to maintain proper pressure.
- Installing 200 zone dampers in supply, return and exhaust branches to control airflow during unoccupied periods.
- Installing control valves in low-pressure steam lines that serve the radiators in the Burrard and Comox buildings.
- Installing occupancy sensors in operating rooms, conference rooms, private dining rooms and the lecture theatre.
- Installing a new cooling tower. Chilled water is piped to the cooling tower instead of sending it to the drain (two more cells need to be added).
- Adjusting flush meters to shorten flush time.
| Energy Type | Units | Savings |
|---|---|---|
| Steam | lb. | 15-21% per year |
| Electricity | peak kW | 9% per month |
| kWh | 15% per year | |
| Water | cu. ft. | 27% per year |
For more information, contact
David MyersLeader, Physical Plant Department
St. Paul's Hospital
1081 Burrard Street
Vancouver BC V6Z 1Y6
Tel.: (604) 806-8273
Fax: (604) 806-8285
E-mail: dmyers@stpaulhosp.bc.ca
Web site: http://www.providencehealthcare.com/info_stpauls_main.html
7.4 Case Study No. 4: The Ottawa Hospital, Civic Campus, Ottawa, Ontario
Overview
The Civic Campus, which was built in 1924, has a current floor area of 167 000 m2 (1.8 million sq. ft.). It operates its own central boiler plant with a high-pressure distribution system and the required certified staff.
Energy Retrofit Measures
Heat Recovery System
A condensing system was installed on the boiler plant exhaust stack. The heat recovered is sufficient to heat all of the ventilation air required for the 9300-m2 (100 000-sq.-ft.) University of Ottawa Heart Institute, which consists mostly of labs and requires close to 100 percent fresh air intake. The recovered heat also supplies a significant portion of the domestic hot water load and helps reduce nitrous oxide (NOx) emissions.
Steam Trap Survey and Retrofit
A steam trap survey found 720 traps, as opposed to the 400 that had been previously documented. Almost $100,000 was spent on trap replacements, for a projected annual energy cost savings of $344,000. Savings could not be positively confirmed because there are not enough meters to isolate the effects. Savings were further masked by the ongoing expansion of the facility.
Winter Cooling System
The hospital's winter cooling system provides cooling for the hospital's chilled water loop. This is the only source of cooling for the water loop when the main chiller plant is shut down for the winter. The winter cooling system circulates glycol through the cooling tower and to a plate heat exchanger that cools the water loop. In the winter, the chilled water loop is used to cool small, high-heat areas such as data centres and, most significantly from a cost perspective, two 75-hp air compressors that supply control air and air for various equipment. Previously, the two screw-type air compressors were cooled by city water (open loop). They are now cooled by the chilled water loop (closed loop), made possible by the winter cooling system. The water savings from this retrofit are therefore more significant than the energy savings. The project is estimated to save about $74,000 per year in water charges.
Direct Digital Controls (DDCs)
DDCs are gradually being retrofitted into existing ventilation systems. Currently, 35 out of the total 84 distinct ventilation systems now have DDCs. Payback periods are usually over five years, making it difficult to get approval for installation on energy savings alone. However, DDCs usually have other more significant benefits, including better control of ventilation systems in areas such as emergency rooms, where 100 percent outside air may be required at a moment's notice.
Future Projects
- A gas turbine cogeneration system with heat recovery worth $6 million, with projected annual energy savings of $800,000, is being considered.
- A lighting retrofit with a simple payback of 4.4 years is being considered. The project is expected to cost $800,000 and save $183,000 per year.
- A project to replace two 60-hp medical air compressors with three new 15-hp compressors is being considered. They would cost $100,000, and annual savings of $52,000 are anticipated due to better load matching. It will be possible to distribute and decentralize compressor locations and increase the reliability of the overall system.
For more information, contact
Brock Marshall, P.Eng.Manager of Energy Systems
Ottawa Hospital – Civic Campus
1053 Carling Avenue
Ottawa ON K1Y 4E9
Tel.: (613) 798-5555, Ext. 6849
Fax: (613) 761-5375
E-mail: bmarshall@civich.ottawa.on.ca
Web site: www.ottawahospital.on.ca
7.5 Case Study No. 5: Cambridge Memorial Hospital, Cambridge, Ontario
Overview
- Built in 1953, Cambridge Memorial Hospital has about 1200 employees and a floor area of 36 000 m2 (388 000 sq. ft.).
- A change in management in 1995 brought a new focus on environmental policies, including energy efficiency.
- A new addition, which is planned for the hospital, will incorporate energy-efficient features and has a goal of using 50 percent less energy than that of a conventional construction.
- The hospital recently achieved ISO 14001 certification (Environmental Management Systems) and reports to be the only hospital in North America with this distinction.
Energy Retrofit Measures
General
- A comprehensive lighting retrofit, including the installation of T-8 lighting, reflectors, ballasts and LED exit lights, is ongoing.
- The building's power factor has been corrected via capacitor banks.
- Tinted windows reduce the building's cooling load.
- Energy bills are being monitored and tracked to minimize billing, especially demand charges.
- Waste incineration has been contracted out, resulting in dollar and energy savings.
Motors
- Fans and pump motors were downsized.
- Efficiency improvements were established.
- Variable speed drives were installed.
- Soft-start starters were installed.
- A future retrofit of elevator motors is planned.
HVAC
- HVAC is now scheduled; equipment is shut down when not needed.
- A water-loop heat pump was installed.
- A program to test steam traps is ongoing.
- A desiccant wheel heat recovery unit is now part of the ventilation system.
Staff Education Programs
- Environmental awareness training is provided to the staff (ongoing).
- Kitchen amenities have been consolidated. (i.e., fridges and ice machines).
- Computers are shut down at night.
- Staff is trained to turn off lights.
ISO 14001 Environmental Management Systems
- "Optimization of Energy Efficiency" is an explicit goal of the hospital's ISO 14001 environmental policy.
- The hospital has an environmental procurement policy.
- The hospital monitors and tracks environmental performance indicators relative to a 1990 baseline, including greenhouse gas emissions.
You can find other buildings publications from the Office of Energy Efficiency. To order paper copies, or to discuss how we can help you make your property more energy efficient, please contact us.
Office of Energy Efficiency
Natural Resources Canada
580 Booth Street, 18th floor
Ottawa ON K1A 0E4
Tel.: 877-360-5500 (toll free)
Fax: 613-947-4121
Web site: http://www.nrcan.gc.ca/energy/efficiency/eefb/buildings/13556 Mary-Jane Hanley
Environmental Coordinator
Cambridge Memorial Hospital
700 Coronation Boulevard
Cambridge ON N1R 3G2
Tel.: 519-621-2333, Ext. 1720
Fax: 519-740-4928
E-mail: mhanley@cmh.org
Web site: www.cmh.org